Ed Dowd, a former Blackrock hedge fund analyst, utilized his expertise in data analysis on Wall Street to generate billions of dollars for his clients. However, in the years following his departure from Blackrock, Dowd conducted ongoing surveillance of economic trends in the US and made a noteworthy discovery. Through his analysis of data on mortality rates pre and post widespread administration of COVID-19 vaccinations using the Vaccine Adverse Event Reporting System (VAERS), Dowd observed a troubling increase in death rates in 2021, particularly among young individuals, unrelated to COVID-19.
As further evidence of his observations, Dowd noted insurance companies sounding an alarm. Scott Davison, CEO of Indiana-based insurer OneAmerica, reported a 40% increase in the death rate among individuals aged 18 to 64 compared to pre-pandemic times. Additionally, Hartford Insurance Group cited a 32% increase in mortality from 2019 and a 20% increase from 2020 before the vaccine was available. Lincoln National also reported a 13.7% year-over-year increase in death claims and a 54% increase in quarter 4 compared to 2019. Further, Dowd pointed out “a spike in mortality among younger, working-age individuals coincided with vaccine mandates. The spike in younger deaths peaked in Q3 2021 when COVID deaths were extremely low (but rising into the end of September).” The same trend followed with disability claims also.
The death and disability data from US government sources lacked the necessary details to understand the specific causes of death or disability. It only indicated whether a person was deceased or disabled – or not. However, Dowd and his research team at Phinance Technologies’ Humanity Project have recently discovered the data they were seeking: the UK Personal Independence Payment database.
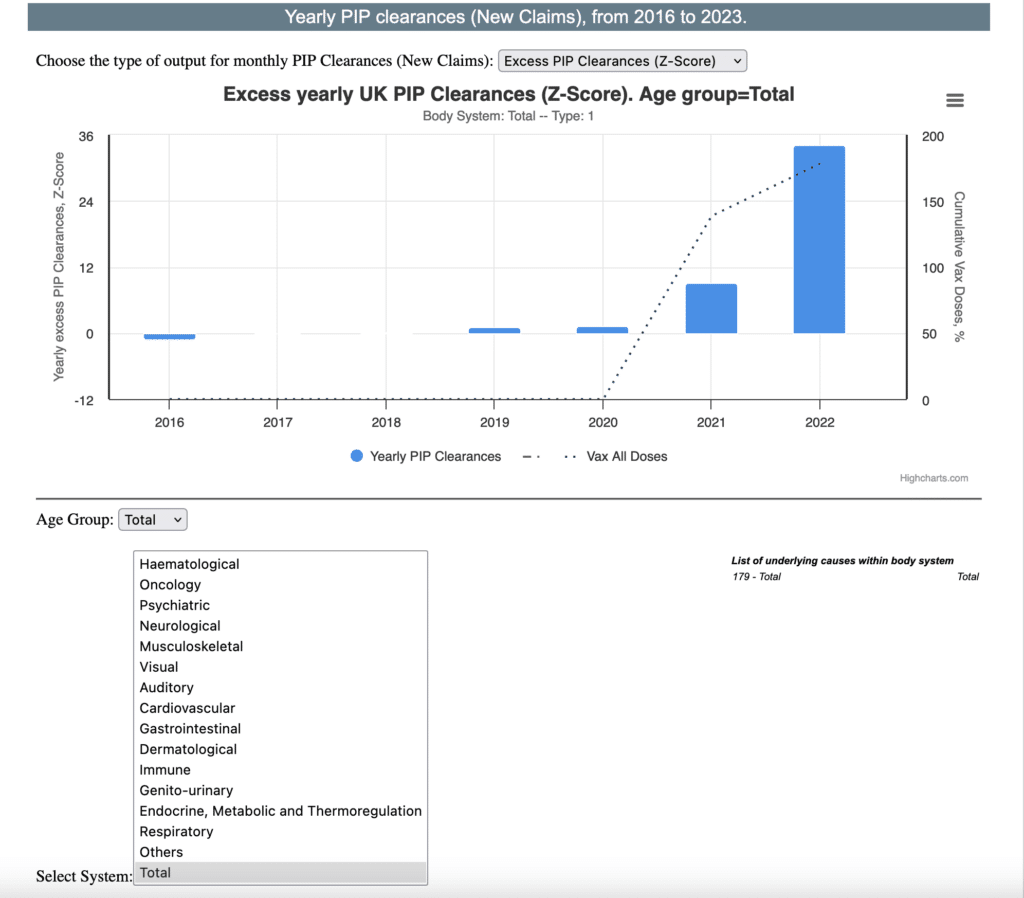
What Dowd and his cohorts found was startling. In their accumulation and analysis of data from 2016 to 2022, they noted what can only be a “Black Swan” event – a wild upward swing in disability by all systems beginning in the first quarter of 2021 – at the same time a global mass vaccination effort began with the debut of an experimental mRNA “vaccine”. In the graph below for all causes and age groups there is a whopping 34 standard deviation increase in disabilities.
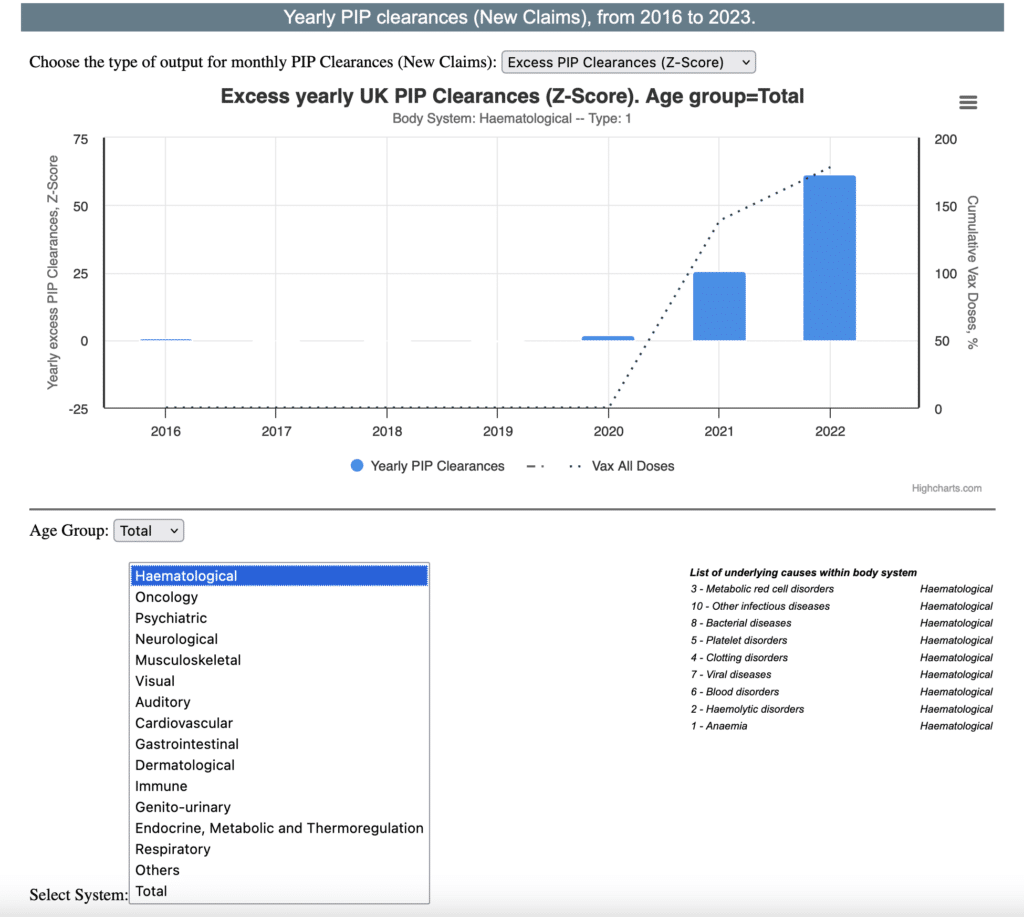
For all ages by hematology disorders, there was a 61 standard deviation increase in disabilities:
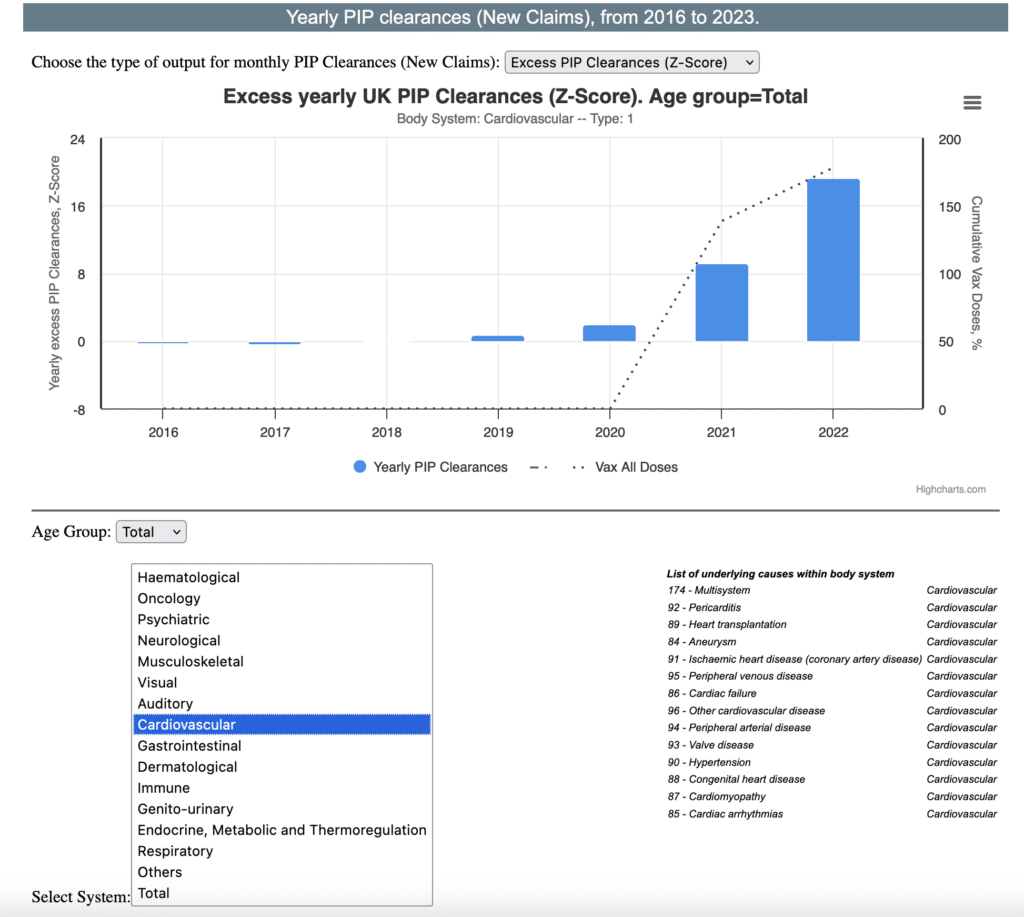
And finally for all ages by cardiovascular disorders, there was a 19 standard deviation increase in disabilities:
Dowd contends these changes in UK disability data are such a large signal they demand explanation. Yet there is none. Again, he points to the global mass vaccination effort with a novel mRNA based “vaccine” as the most likely culprit. And he contends the same trend in likely occurring here in the US based upon previous analyses.
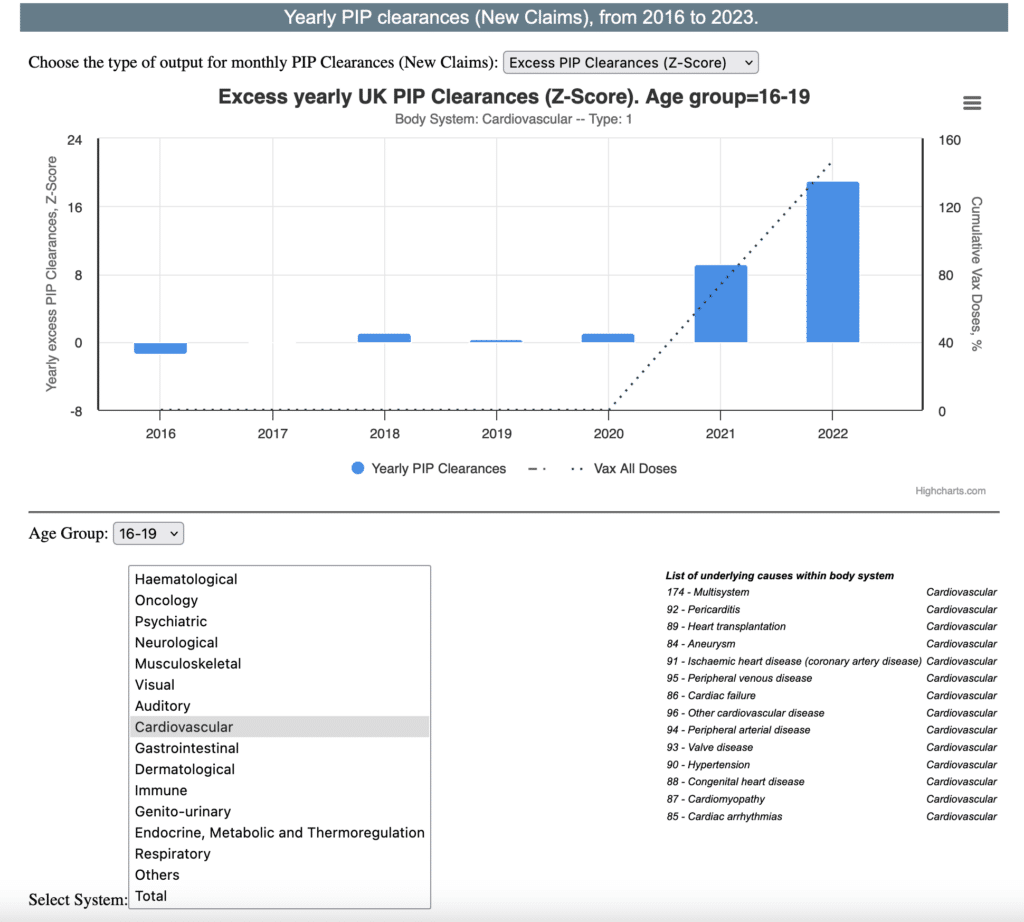
My personal concern for those of us in Dentistry is focused on office based anesthesia. In the age cohort between 16-19 years of age – specifically that population undergoing routine, prophylactic M3 surgery – there is a 19 standard deviation increase in cardiovascular disabilities – including pericarditis near the top of all causes:
I cannot speak for anyone other than myself – but this is frightening. Brief periods of hypoxia – triggers for ventricular irregularity – are not uncommon in dental anesthesia. If myocarditis increases ventricular irritability, surely more frequent episodes of ectopy ventricular tachycardia, or even ventricular fibrillation could ensue.
I am no longer administering general anesthesia but I ask myself frequently what I would be doing now – armed with this kind of data – if I were? First of all, and I credit Peter McCollough MD MPH for his expertise, I think I would start with the history of COVID vaccinations – how many and which lots? The more vaccinations, the greater the risk. Further, we know from Craig Paardekooper’s work on the toxicity associated with different batches of all COVID mRNA manufacturers, some are worse than others. Physical evaluation and ECG noting any ST or PR segment alterations – with special note to gender – young, athletic males are at risk. Then, if the index of suspicion is great enough key labs such as troponin for myocarditis, d-dimer for micro-clotting, CBC, CMP, and imaging such as cardiac MRI and pulmonary chest CT angiogram could be considered. Recent case reports also suggest that myocarditis may relapse over time.
The knowledge base regarding the COVID mRNA vaccines continues to grow. Contrasted to the rollout in early 2021 we now know the lipid nanoparticle (LNP) delivery system has it’s own toxicity independent of payload – nor does it stay at the site of injection. A recent article in Science Immunology showing that vaccine-induced myocarditis is likely driven by the platform (LNP) & not antigen specific (i.e., spike protein) – implying that future mRNA-based vaccines/drugs would have same risk!
The insertion of pseudouridine to the mRNA while increasing it’s stability also increases it’s biological half-life far longer than the public had been advised. Reverse transcription to host DNA has been proven. Furthermore, research on behalf of Kevin McKernan has demonstrated that the Process II synthesis of mRNA using E Coli plasmid (as opposed to the “cleaner” synthetic Phase I PCR process) has consistent quality control problems resulting in segments of double stranded DNA contaminating the product – in addition to the identification of an SV40 (simian virus 40) promoter segment which can promote oncogenesis. Unlike mRNA, double stranded DNA does not require an intermediate step to integrate into host DNA. Lastly, bacterial endotoxin is a known contaminate of harvesting the mRNA product from E Coli and many of the toxicities of the product appear to be potentiated by it’s presence.
Because the mRNA segment as well as plasmid DNA can be integrated into the host genome, the effects of the spike protein do not necessarily wane, rather they may continue to build depending upon production lot. It’s a bit like russian roulette, but the impact of exposure should become apparent to the reader.
With the ever increasing reports of high profile, vaccinated adults who are otherwise healthy experiencing cardiac arrest a growing sense of caution would seem appropriate. I know of several oral & maxillofacial surgeons who are witnessing increased cardiac abnormalities in patients who are under evaluation for office based surgery and increased incidence of ectopy during surgery. I hope and pray for no untoward events, but since there are indications the toxic effects of the COVID mRNA vaccines do not wane, the ever growing body of evidence suggests that a more circumspect approach to office based anesthesia may be in order. In consideration of the significance of Dowd’s UK PIP analysis, I believe, one must assume the presence of myocarditis, rather than the alternative.
David MH Lambert, DDS
Diplomate, ABOMS